
Article / Case Study
1Department of Neurosurgery North –Pest Medical Center, Military Hosp. Budapest , Hungary.
2 Southern Methodist University Dallas Texas.
3 Department of Neurosurgery, St. John’s Hospital, Budapest, Hungary.
4Semmelweis University Budapest, Hungary
András Csókay MD. Ph.D.
Chief of Department of Neurosurgery North-Pest Central
Hospital,
Military Hospital, Str.44.Róbert K.,
Budapest H-1334,
Hungary
14 May 2023 ; 7 June 2023
The work presented on EANS 2020 Beyond Borders Virtual Congress
There is considerable literature on the harmful effects of distress in medically critical situations. There is just as much literature available on psychological methods aimed at relieving stress. One can make creative and fast decisions without stress much more effectively. We will discuss these acute decisions and investigate them with a scientific approach, attempting to judge the propriety of decisions made in emergencies by medical personnel. We will investigate the results of our contemplative approach to this phenomenon through concrete examples.
Deliberate practice of contemplative behavior daily gives one the ability to quickly retrieve the learned approach, previously studied and experienced in contemplative behavioral practice, during a given procedure. Once the information is retrieved regarding a certain procedure, it can be synthesized with the situation at hand, which allows for the formulation of an enhanced creative option that may increase the possibility of a successful procedure. Thus, the procedure together with the application of the contemplative approach could be acknowledged as a real innovative treatment after gaining scientific approval. This article gives an account of the application of the practiced contemplative approach during a craniopagus, resulting in the success of the procedure.
The article gives an account of three different neurosurgical innovations that were possible with the application of the contemplative approach. These innovations eventually gained wide recognition, applied by many, leading to progress in neurosurgical challenges not conquerable before. The case study we investigate was the separation of a craniopagus in which the engraved spiritual algorithms of the stress-distress situation there because of contemplative practice led to the innovation of surgical techniques responsible for the success of the procedure.
Spiritual silence is a helpful aid, swiftly attainable if the invocation of it is practiced every day. Ensuring the presence of spirituality during the mindful contemplation of procedures results in professional success of emergencies, demonstrated in the case of the neurosurgical separation of a craniopagus. Alongside a strong intellectual understanding of the profession, emphasis on spirituality allows for successful execution.
Keywords : distress situation, craniopagus, conjoined twins, fresh cadaver, contemplation
There is a very extensive availability of medical literature detailing the harmful effects of distress on decisions made in acute medical situations. (Allport & Ross, 1967; Chen et al., 2016; Bernardi et al., 2001; Bechara et al., 2000; Heyhoe et al., 2016; Henriksen et al., 2020; Bucknall, 2003; Emmons, 1999). Equally vast is the literature on psychology and spirituality as it pertains to this concern; solutions include medicaments, practicing mindfulness, meditation (Bernardi et al., 2001; Emmond, 2000; Allport & Ross, 1967; Emmons, 1999; Ekman et al., 2005; Fredrickson & levenson, 1998) and prayer. These techniques help to employ creative and effective decisions when the opportunity arises. It often occurs that generally accepted solutions to procedures must be ignored, for they might not offer solutions to the specific problem encountered. Alternative decisions made in emergencies can be later examined through scientific methods and verified that they were medically correct and effective over the convention. (Astrow et al., 2001; Geoffrey et al., 2015; Garfinkel et al., 2016; Heyhoe et al., 2016; Henriksen et al., 2020; Holland et al., 2017) Principles of bioethics permits deviation from conventional methods and the use of situational solutions which arise from “scientific rationale.”(Warren, 1999) Eventually, these alternative solutions may even be accepted as the standard. In neurosurgery and other specialties alike, numerous decisions are made based off this situational rationale.
The 24-hour surgical separation of the craniopagus twins as well as the post-operative phase presented many situations in which the application of situational judgement was made necessary.
Conscious and deliberate practice of contemplation on a daily basis enables one with the ability to, in acute situations of distress, be calm and collected. Synthesizing the information practiced and learned with the circumstances one is presented with allows a creative option for the procedure to be invented, which after being reviewed and accepted can result in real innovative progress. The connections of the cortex and subcortical structures is the neuroanatomical substrate of the process mentioned above, where the recall of information is modulated by electrochemical signals from the hippocampus/limbic system. (Kusev et al., 2017; Bechara et al., Bechara et al., 2003).
Neuroscientists agree that our emotions and motivations arise from activity in neural pathways present in the deeper brain structures. The greater the activation of these pathways, the greater the number of emotional perceptions, this activation being necessary for the quick recall of stored information in familiar situations.
Put simply, we never forget events, even those in our distant childhood, that have some deep emotional connection attached to them. The creation of this rich, inner emotional world is enhanced by meaningful artistic experiences, mindfulness, meditative prayer, and contemplation, whereby practicing these techniques, we can better access this inner spiritual cocoon of enhanced emotionalism in the exploration of which we find otherwise unavailable opportunities and perhaps profound scientific truths (Csókay et al., 2002; Csókay et al., 2009; Csókay et al., 2013; Csókay et al., 2019). We will give a testament to the value of practicing the above-mentioned contemplative approach as it pertains to the field of neurosurgery.
We refer to three distinct neurosurgical innovations in medical literature that have acclaimed wide acceptance and application, which we have explained and brought to light in multiple international forums in the past (Csókay et al., 2002; Csókay et al., 2009; Csókay et al., 2013; Csókay et al., 2019). The ideas for these innovations were born in deep Jesus (rosary) prayer. (Csókay et al., 2022).
The case most worthy of mentioning was the neurosurgical separation of three-year-old craniopagus twins done about 4 years ago by the authors of this publication (Csókay et al., 2022). The algorithmic management of the multitude of life-threatening circumstances encountered during the neurosurgical portion of the separation has been detailed in the only article published since the surgery (Csókay et al., 2022). In this article we will focus on the successes arising from the innovative neurosurgical solutions obtained during contemplative prayer.
In our first encounter with the Siamese twins, a noticeable and insurmountable pressure was felt by the neurosurgical team, confounded by optimistic expectations of a successful separation. While inspecting the immense magnitude of the shared venous systems between the twins (Figure 1 a,b), we immediately understood why even the most experienced of neurosurgeons were unwilling to undertake the operation. If we give a shared vein to one of the twins, the other one most certainly dies. If that was the case, the operation cannot be taken on. After 10 minutes of deep contemplation of Jesus prayers, a solution began to appear, giving us an idea to pursue a scenario in which the shared venous system was distracted from both twins. We knew that the third author, a highly experienced endovascular specialist, successfully completed this task in the past using what is known as a balloon occlusion test series.
 Figure 1(a): Difficult Situation of Craniopagus Case
Figure 1(a): Difficult Situation of Craniopagus Case
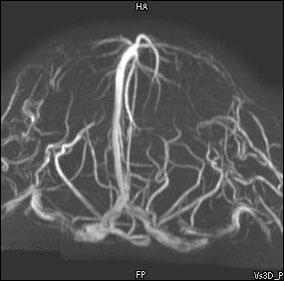 Figure 1(b): The Common Venous System Seemed Like an Unsolvable Problem
Figure 1(b): The Common Venous System Seemed Like an Unsolvable Problem
Since venous blood had more difficulty of flow towards the collateral veins because of the clogged common sinuses, extremely persistent bleeding developed from the congested bridge veins during the open surgery. For the separation of the twins to be completed, these veins had to be irreversibly removed from the shared clogged sinuses. This procedure was made extremely difficult from the reactive brain edema which developed during the operation. In a span of second, the twins were in a hemodynamically critical condition induced by the continuous blood loss. While in Jesus prayers contemplation, a “multilayer tampon” solution was bestowed upon me to this increasingly dangerous problem, because of which we were able to control the persistent venous bleeding unstoppable merely using bipolar coagulation.
The portion of the operation executed on sides of the brain not shared went relatively fast, we finished in about 12 hours (Figure 2a, b,c). After the rotation, we ran into an undesired circumstance. We practiced on nearly 300 cadavers the maneuvers involved in regions where the sulci morphed into each other much like a hand in a glove. We were looking for sulci where the separate gyri had embedded into one another. However, during the operation, the sulci had adhered to one another more intensely than we anticipated, largely due to the substantial loss of cerebrospinal fluid. We could hardly move forward, despite using the waterjet technique and the ultramicroscopic technique of finger tip support (Csókay et al., 2009; Csókay et al., 2013; Csókay et al., 2019). A couple of hours passed before we conclusively realized that separation of the side in question was not possible without causing trauma to the cortex. In addition, we were also facing persistent bleeding, creating a situation we did not encounter on other sides of the brain; this was happening all the while the increasing length of the surgery, coupled with considerable amounts of blood transfusions, was exponentially increasing the risk of complications from the transfusion itself and making adverse reactions due to the development of septic brain tissue more likely.
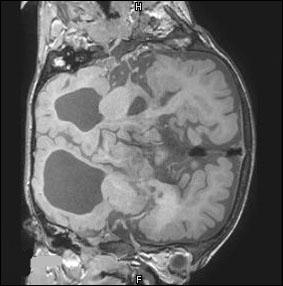 Figure 2(a): The Separation of Interdigitated Gyri were also a Difficult Microsurgical Task
Figure 2(a): The Separation of Interdigitated Gyri were also a Difficult Microsurgical Task
 Figure 2(b): 3D Models Helped to Imagine The Real Situations
Figure 2(b): 3D Models Helped to Imagine The Real Situations
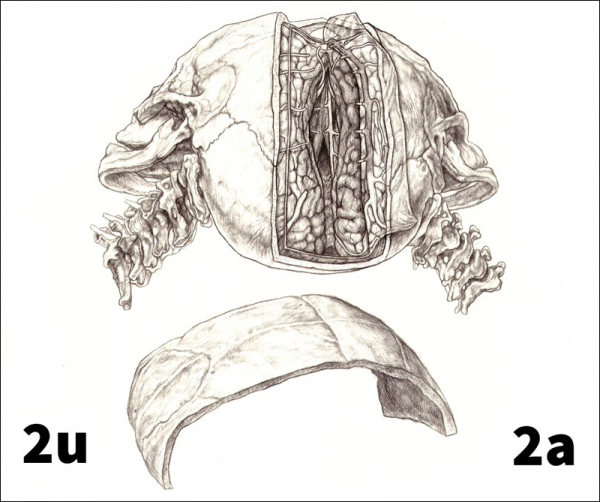 Figure 2(c): Drawing of Separation
Figure 2(c): Drawing of Separation
As it had in the past, contemplation Jesus prayers helped us to listen to our inner intuition. It had told to first author to speed up and sacrifice the trauma to the cortex so that we could move on; we had no choice but to trust that the neuroplasticity of the kids would allow them with exceptional regeneration. With that decision, we were able to finish the surgery in 25 hours and hand over the kids to the plastic surgery team for closing. Our presumptive decision to move forward turned out to be the right choice, because after 10 days, despite the cortical hemorrhage, one of the kids began to move her extremities on the contralateral side.
After the surgery, we faced the possibility of vegetative state developments more than once, presenting acute life-threatening situations. This was the case despite applying the recommended 30 degree incline for patients suffering cranium injuries. While contemplating the solution to this problem, I once again concluded and realized that an unorthodox method might better suit the twins: laying down horizontally or in a minimal Trendelenburg position. With this unorthodox solution, the brainstem, which was subject to torsion, could be in a mechanically stabilized position. The anesthesiologists came to the same conclusion Independent of the neurosurgical team, and after having applied this alternative position, the results were satisfactory and the vegetative tendencies of the children gradually stabilized.
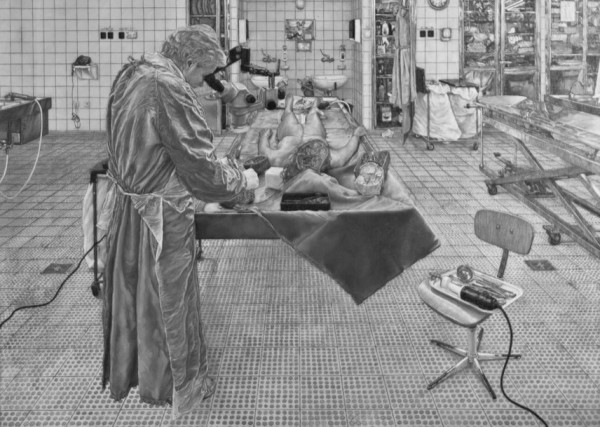 Figure 3: More than 300 fresh cadaver practice helped to obtain the skills. Jesus prayers helped us to spent a lot of time day by day in autopsy room.
Figure 3: More than 300 fresh cadaver practice helped to obtain the skills. Jesus prayers helped us to spent a lot of time day by day in autopsy room.
On the 33rd day after the surgery, one of the twins suffered a very serious brain hemorrhage. This most likely happened because of incompetent cranium reconstruction (Fig.4), which arose because of a professional misunderstanding that resulted in the reconstruction not being done by the neurosurgical team, who tirelessly practiced the procedure on cadavers and 3D models prior to the surgery. As a result, one of the twins is in GOS5 and the other in GOS3 rehabilitation to this day. (Fig.5)
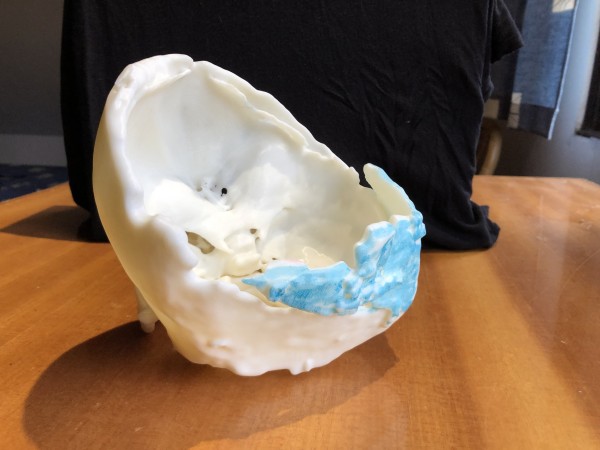 Figure 4: The insufficient posterior bone protection
Figure 4: The insufficient posterior bone protection

Figure 5: Twins 3 months after the separation
A brain that has undergone hemorrhage is very sensitive; this impeded our ability to effectively repair the dura in an atraumatic way during the cranioplasty. Through contemplation, it became increasingly clear that we had no choice but to embark on a maneuver, normally performed with the naked eye, under 20x magnification of a microscope. The successful application of this maneuver allowed us to salvage the sensitive hemisphere of the brain from even minimal trauma.
The ability to tap into a peaceful and silent state of the soul in times of its necessity is only possible through daily spiritual practice. In this article, we demonstrated the benefit of mindful contemplation in the field of neurosurgery. The multitude of critical decisions made during the separation of the craniopagus twins unquestionably proves its use. Alongside a cultivated professional understanding and skillset, it is critical to emphasize spirituality, so that we can transcend situations of distress, and make good, innovate acute decisions when prompted.(Fig.6.)
 Figure 6: Mystic drawing Jesus in the OR
Figure 6: Mystic drawing Jesus in the OR
Specifically, we would like to express ourgratitude to: László Nagy MD. (Pediatric Neurosurgeon, Health Science Center Lubbock, USA) for medical advice Enikő Czirják Chief (scrub nurse) BalázsSándorMuhari-Pap (painter) for the medical illustrations Éva Petrik – Medical Illustrator JánosSzász (film director) leadingthe film footage from 4 camera positions. BertalanTóth and Júlia Szonja Bácskai for video-editing Zoltán Kiss (film sculptor and model maker) for making doll models which was one of the main base of practiceand analytic way of thinking József Pejkó (autopsy assistant) helpingus during the daily inductive fresh cadaver excersises Márta Jackel MD. (Cheaf ofPathologyDept.) for providing background for daily cadaveric practice Fr.Szabolcs Sajgó (Society of Jesus) Director of the House of Dialogue–(spiritual leader of the hungarian participants) for giving specific moral support by teaching us the contemplative prayer of Jesus. The nuances and analysis of complications described in the paper were born during these prayers. Thousands of spiritual and monetary donors There are numerous hospitals, companies, and individuals from Bangladesh and Hungary that we wish to thank for their contributions to this work
- Allport, G., & Ross, J. (1967). Personal religious orientation and prejudice. Journal Personal and Social Psychology, 5(4), 432-43. DOI: 1037/0022-3514.5.4.432
- Chen, S-L., Hsu, H-Y., Chang, C-F., & Lin, EC-L. (2016). An exploration of the correlates of nurse practitioners’ clinical decision-making abilities. J Clin Nurs, 25(7-8), 1016–1024. DOI: 1111/jocn.13136
- Bernardi, L., Sleight, P., Bandinelli, G., Cencetti, S., Fattorini, L., Wdowczyc-Szulc, J., & Lagi, A. (2001). Effect of rosary prayer and yoga mantras on autonomic cardiovascular rhythms: comparative study, BMJ, 323(7327), 1446–1449. DOI: 1136/bmj.323.7327.1446
- Bechara, A., Damasio, H., & Damasio, A. R. (2000). Emotion, decision making and the Orbitofrontal cortex. Cereb Cortex, 10(3), 295–307. DOI: 1093/cercor/10.3.295
- Heyhoe, J., Birks, Y., Harrison, R., O’Hara, J. K., Cracknell, A., & Lawton, R. (2016). The role of emotion in patient safety: are we brave enough to scratch beneath the surface? J R Soc Med, 109(2), 52–58. DOI:1177/0141076815620614
- Henriksen, D., Richardson, C, & Gradisar, M. (2020). Mindfulness and creativity: Implications for thinking and learning. Think Skills Creat, 37, 68-69. DOI: 1016/j.tsc.2020.100689
- Bucknall, T. (2003). The clinical landscape of critical care: nurses’ decision-making. J Adv Nurs, 43(3), 310–319. DOI:1046/j.1365-2648.2003.02714.x
- Emmons, R. A. (1999). The psychology of Ultimate Concerns: Motivation and Spirituality in Personality. Guilford Press, New York. Retrieved from https://www.guilford.com/books/The-Psychology-of-Ultimate-Concerns/Robert-Emmons/9781572309357
- Emmond, R. A. (2000). Is spirituality an Intelligence? International Journal for Psychology of Religion. 10(1), 3-16. DOI:1207/S15327582IJPR1001_2
- Ekman, P., Davidson, R. J., Ricard, M., Wallace, A. (2005). Buddhist and Psychological Perspectives on Emotion and Well Being. Current Direction in Psychological Science. 14(2), 39-63. DOI:1111/j.0963-7214.2005.00335.x
- Fredrickson, B. L., & levenson, R.W. (1998): The question:’Does religion /or spirituality/ cause physicalhealth Benefits?’ Journal of Personality and Social Psychology, 54, 432-443.
- Astrow, A. B., Puchalski, C. M., Sulmary, D. P. (2001). Religion, Spirituality and Health Care: Social, Ethical and Practical Considerations, American Journal Medicine, 110(4), 283-7. DOI: 1016/s0002-9343(00)00708-7
- Geoffrey K. Lighthall, M., & Vazquez-Guillamet, C. (2015). Understanding Decision Making in Critical Care. Clin Med Res, 13(3-4), 156–168. DOI: 3121/cmr.2015.1289
- Garfinkel, S. N, Zorab, E., Navaratnam, N., Engels, M., Mallorquí-Bagué, N., Minati, L., Dowell, N. G., Brosschot, J. F., Thayer, J. F., & Critchley, H. D. (2016). Anger in brain and body: the neural and physiological perturbation of decision-making by emotion. Soc Cogn Affect Neurosci, 11(1), 150–158. DOI:1093/scan/nsv099
- Holland, A., Dooley, G., Fedock, B., Susan, F., & Liston, B. (2017). Meditation, mindfulness, and critical thinking: individual characteristics in online higher education. J Psychol Cognition. 2(3), 170-176. Retrieved from https://www.alliedacademies.org/articles/meditation-mindfulness-and-critical-thinking-individual-characteristics-in-online-higher-education.pdf
- Warren T. (1999). Reich Encyclopedie of Bioethics. New York: Raven Press; 1999 p. Retrieved from https://www.worldcat.org/title/encyclopedia-of-bioethics/oclc/31290994
- Kusev, P., Purser, H., Heilman, R., Alex, J. C., Paul, V. S., Victoria, B., Rose, M., & Peter Ayton. (2017). Understanding risky behavior: the influence of cognitive, emotional and hormonal factors on decision-making under risk. Front Psychol, 8(102), DOI:3389/fpsyg.2017.00102
- Bechara, A., Damasio, H., & Damasio, A. R. (2003). Role of the Amygdala in decision-making. Ann N Y Acad Sci, 985(1), 356–369. DOI: 1111/j.1749-6632.2003.tb07094.x
- Csókay, A., Együd, L., Nagy, L., & Pataki G. (2002). ”Vascular tunnel creation” to improve the efficacy of decompressive craniectomy in post-traumatic cerebral edema and ischemic stroke. Neurol, 57, 126-129.
- Csókay, A., Valálik, I., Jobbágy, Á. (2009). Early experiences with a novel technique in the course of micro neurosurgery. Surg Neurol, 71(4), 469–472. DOI: 1016/j.surneu.2008.05.003
- Csókay, A., Papp, A., Imreh, D., Czabajszky, M., Valálik, I., & Antalfi, B. (2013). Modelling pathology from autolog fresh cadaver organs as a novel concept in neurosurgical training. Acta Neurochir, 155(10), 1993–1995. DOI: 1007/s00701-013-1727-8
- Csókay, A., Josvai, A., Csókay, G., & Jackel, M. (2019). The Importance of Daily Fast Fresh Cadaver Dissection (How can we organize it?). J Neurol Stroke, 9(1), 1‒3. DOI: 15406/jnsk.2019.09.00336
- Csókay, A., Hudák, I., Valálik, I., Jósvai, A., Trencséni, B., Égető, E., Csókay, G., & Tóth, B. (2022). Neurosurgical Steps and Lessons Learned in Final Separation of 3-Year-Old Craniopagus Twins. World Neurosurgery, 164, 290. DOI: 1016/j.wneu.2022.05.065
- Kozlowski, D., Hutchinson, M., Hurley, J., Rowley, J., & Sutherland, J. (2017). The of emotion in clinical decision making: an integrative literature review. BMC Med Educ, 17(1), DOI: 10.1186/s12909-017-1089-7
- Lauri, S., & Salanterä, (2002). Developing an instrument to measure and describe clinical decision making in different nursing fields. J Prof Nurs, 18(2), 93–100. DOI: 10.1053/jpnu.2002.32344
- Ledger, U., Reid, J., Begley, A., Prior, L., McAuley, D., & Blackwood, B. (2021). Moral distress in end-of-life decisions: A qualitative study of intensive care physicians. J Critical Care, 62, 185-189. DOI: 1016/j.jcrc.2020.12.019
- Koenig, H. G. (2009). Research on religion, spirituality, and mental health: A review. Can J Psychiatry, 54(5), 283–91. DOI: 1177/070674370905400502
- Koenig, H. G., McCullough, M. E., & Larson, D. B. (Eds). (2001). Handbook of Religion and Health. Oxford University Press, Oxford. https://doi.org/10.1093/acprof:oso/9780195118667.001.0001
- Masters, K. S., & Spielmans, G. I. (2007). Prayer and Health: Review, Meta-Analysis, and Research Agenda. Journal of Behavioral Medicine,30(4), 329-38. DOI: 1007/s10865-007-9106-7
- Ramon Moraes Penha, & Maria Júlia Paes da Silva. (2012). “Meaning of spirituality for critical care nursing.” Texto Contexto Enfermagem, 21(2), 260–68. DOI:1590/S0104-07072012000200002