
Article / Case Report
KK Women’s and Children’s Hospital, 100 Bukit Timah Road, Singapore 229899.
Jia Ying Chong,
KK Women’s and Children’s Hospital,
100 Bukit Timah Road,
Singapore 229899.
31 Jan2024 ; 24 February 2024
Microperforate hymen is a rare anomaly which affects the quality of life and sexual activity of young women. We present a surgical technique for the treatment of microperforate hymen.
We report a 30-year-old nulliparous lady who presented with vaginismus, intermenstrual bleeding and menorrhagia. Physical examination revealed a pinpoint hymenal membrane opening at 12 o’clock position. The patient underwent hymenectomy and hysteroscopy with dilatation and curettage. Two Foley catheters were used: one was inserted into the urethra, the other into the vagina via the hymenal opening. Bulb of the vaginal catheter was inflated to demarcate hymenal membrane from urethra to prevent urethra injury during the hymenectomy. A cruciate incision was made over hymen membrane. Recovery was unremarkable, and patient was able to have sexual intercourse.
This case highlights the importance of performing a thorough genital examination to identify anomalies. Early surgical intervention prevents complications and improve affected women’s quality of life.
Keywords: Microperforate hymen, vaginismus, hymenal anomalies.
Female genital tract anomalies can significantly impact a woman’s somatic function (e.g. menstrual hygiene), sexual activity and quality of life. The hymen is a thin fold of membrane which marks the distal most extent of the vagina and the most proximal boundary of the vulvar vestibule[1]. Failure of the hymen to perforate completely in the perinatal period can lead to varying anomalies, including imperforate, microperforate or septated hymen[2]. Microperforate hymen is a rare congenital subocclusive anomaly which results from an incomplete canalisation of the fetal hymen, usually occurring shortly before birth. Its exact incidence rate is unknown[3]. It usually is an isolated anomaly. However, it can be associated with other anomalies such as bifid clitoris, vaginal septa, duplicate ureter, imperforate anus and other anorectal malformations[3,4,5].
Females affected with microperforate hymen often have delayed diagnosis during the post-pubertal period as it is only a partially obstructive anomaly compared to an imperforate hymen[6]. They often present with recurrent urinary, genital tract or pelvic infections, vaginismus or irregular menstrual periods[6,7].
A thorough genital examination, high clinical suspicion and recognition of symptoms from microperforate hymen can lead to prompt diagnosis and early surgical intervention. Early intervention improves the woman’s quality of life and prevents potential complications and sequelae, such as recurrent genitourinary infections, sepsis, haematometra, pyocolpos, endometriosis and long-term psychological and sexual health problems.
A 30-year-old Chinese lady presented to the outpatient Gynaecology clinic complaining of vaginismus, intermenstrual bleeding and menorrhagia. She was married but nulliparous, as she could not have sexual intercourse due to severe vaginismus. She had difficulty with both digital and penile penetration. She had regular monthly menses, heavy flow on days 2 to 3 of the menstrual cycle, and intermenstrual bleeding. She did not have dysmenorrhoea. Her general physical examination was unremarkable. She had normal secondary sexual characteristics. A gynaecological examination revealed an intact hymenal membrane with a pinpoint hymenal opening at the 12 o’clock position (Figure 1). A thin cotton swab could be inserted through this hymenal opening with no blockage felt across the length of the vagina. A transabdominal ultrasonography scan of the pelvis showed a normal uterus with normal endometrial thickness. Both ovaries were normal, with no adnexal masses. The impression was a microperforate hymen.
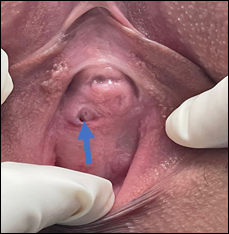 Figure 1: Microperforate hymen with a pinpoint size of the hymenal opening at the 12 o’clock position (indicated by the blue arrow).
Figure 1: Microperforate hymen with a pinpoint size of the hymenal opening at the 12 o’clock position (indicated by the blue arrow).
The patient underwent hymenectomy, diagnostic hysteroscopy, dilatation and curettage under general anaesthesia. Two Foley catheters were used: one was inserted into the urethra and the other into the vagina via the hymenal opening (Figure 2). The bulb of the vaginal Foley catheter was inflated with 5 millilitres (mls) of sterile water to help demarcate the hymenal membrane from the urethra, thereby helping to prevent inadvertent urethra injury during the hymenectomy. (Figure 3). A cruciate incision (Figure 4) was made over the hymen membrane.
 Figure 2: One Foley catheter was inserted into the vagina through the hymenal opening while another Foley catheter placed into the urethra
Figure 2: One Foley catheter was inserted into the vagina through the hymenal opening while another Foley catheter placed into the urethra
 Figure 3: Cruciate incision was outlined over the hymen
Figure 3: Cruciate incision was outlined over the hymen
 Figure 4: Cruciate incision was made over the hymen
Figure 4: Cruciate incision was made over the hymen
In an interrupted fashion, the vaginal mucosal edges were marsupialised using absorbable braided sutures (Vicryl Rapide™ 2.0) (Figure 5). These aid in haemostasis and prevent hymen re-closure via adhesions or scarring. The size of the introitus opening was adequate for sexual intercourse. A speculum examination done post-procedure revealed a normal cervix and vagina. Diagnostic hysteroscopy revealed thickened endometrium with bilateral ostia seen and a normal endocervical canal. She was discharged well on the same evening. Postoperatively, she was covered with oral amoxicillin/clavulanic acid for 5 days, oral analgesia and topical lignocaine gel. She was also given sitz bath and perineal hygiene advice.
 Figure 5: Mucosal edges were then reapproximated using absorbable sutures in an interrupted fashion for haemostasis and prevention of hymen reclosure.
Figure 5: Mucosal edges were then reapproximated using absorbable sutures in an interrupted fashion for haemostasis and prevention of hymen reclosure.
She was subsequently reviewed in the clinic 2 weeks later, and the patient had an uneventful recovery. She had no urinary or bowel issues. Her menstrual flow was back to normal. On examination, the wound was well healed (Figure 6) and she could have both speculum and vaginal examinations performed. The patient was advised to use lubrication and attempt digital penetration first.
 Figure 6: Wound review 2 weeks after the operation
Figure 6: Wound review 2 weeks after the operation
She was reviewed again 6 weeks postoperatively, and the patient was able to have digital penetration. The hymen ring had healed completely and the introitus was normal (Figure 7).
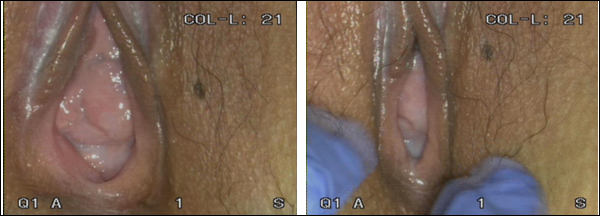 Figure 7: Wound review 6 weeks after the operation
Figure 7: Wound review 6 weeks after the operation
Microperforate hymen is a subocclusive hymenal anomaly; hence, its symptoms can vary among affected women depending on the size of the opening of the hymen. Affected women are often able to have menstrual efflux as the pinhole opening of the hymen can still permit the passage of fluids. Hence, the diagnosis of microperforate hymen may be only made during the post-pubertal period when they present to the clinic with vaginismus or recurrent genitourinary infections[3].
Recurrent urinary tract infections can occur due to the pooling of urine in the functional urogenital sinus and result in an ascending infection of the urethra.8 Affected women may also present with recurrent lower genital tract or pelvic infections and may develop pyocolpos[3,7]. Subocclusive hymenal anomalies such as microperforate hymen can also interfere with vaginal intercourse and affect sexual health. Depending on its severity, it may be associated with subfertility.
A careful and detailed history taking and clinical examination, including a thorough genital examination, should be undertaken when young females present with genitourinary complaints, vaginismus or irregular menstrual bleeding. Radiological evaluation with an ultrasonography scan of the pelvis can aid in completing the evaluation.
Treatment of microperforate hymen is often surgical correction of the anomaly, and the most common techniques include a cruciate or U-shaped incision of the hymen[3,9,10]. We present a surgical technique to help reduce the risk of injury to the urethra during hymenectomy. By inserting the two Foley catheters, as demonstrated in Figure 2 and inflating the bulb of the vaginal catheter, it demarcated the area on which the cruciate incision was made. It distends the hymen membrane and allows the surgeon to determine the superior aspect of the cruciate incision to avoid inadvertent injury to the urethra. Redundant hymenal mucosa is excised, and mucosal edges reapproximated using absorbable suture interrupted for haemostasis and prevention of hymen re-closure[9,10].
A less invasive method, i.e. serial dilation of the microperforate hymen with Hegar dilators, had been reported in the literature[10]. However, the two cases reported did not have obstructive symptoms or a history of genital tract infections which may suggest that the hymenal opening may not be as severe. Moreover, the long-term success in restoring menstrual and sexual functions is unknown with this technique[3,11].
Subocclusive anomalies of the hymen, such as microperforate hymen, are rare and hence often overlooked, and diagnosis is usually delayed. A high index of suspicion is paramount when a young lady presents with irregular menstrual bleeding, recurrent genitourinary infections or vaginismus. Surgical management is recommended for such anomalies to prevent long-term complications and significantly improve the affected woman’s quality of life. We recommend our surgical technique to reduce the risk of injury to the urethra during hymenectomy.
We have no conflicts of interest to disclose.
- Kumar V, Kumar KV, Krishnamurthy KH, Kumar R. A Rare Case Report of Microperforate Hymen with Difficulty in Penetration. J South Asian Feder Menopause Soc. 2014;2(2):97-98. DOI: 10.5005/jp-journals-10032-1052
- Miller RJ, Breech LL. Surgical Correction of Vaginal Anomalies. Clin Obstet Gynecol. 2008 June;51(2):223-236. DOI: 10.1097/GRF.0b013e31816d2181. PMID: 18463454.
- Tardieu SC, Appelbaum H. Microperforate Hymen and Pyocolpos: A Case Report and Review of the Literature. J Pediatr Adolesc Gynecol. 2018 Apr;31(2):140-142. DOI:10.1016/j.jpag.2017.08.006. Epub 2017 Aug 31. PMID: 28838865.
- Winderl LM, Silverman RK. Prenatal diagnosis of congenital imperforate hymen. Obstet Gynecol. 1995 May;85(5 Pt 2):857-60. DOI: 10.1016/0029-7844(94)00405-3. PMID: 7724137.
- Suidan FG, Azoury RS. The transverse vaginal septum: a clinicopathologic evaluation. Obstet Gynecol. 1979 Sep;54(3):278-83. PMID: 471367.
- Ferrarini OMF, Munhoz LO, Simões RS, Cezarino PYA, Mieli MPÂ, Margarido PFR, Guida FJ, Baracat EC. Microperforated hymen: a case of delayed diagnosis. Autops Case Rep. 2014 Sep 30;4(3):59-63. DOI: 10.4322/acr.2014.030. PMCID: PMC5444400. PMID: 28573120.
- Sanfilippo AM, Mansuria SM. Microperforate hymen resulting in pelvic abscess. Journal of pediatric and adolescent gynecology. 2006 Apr;19(2):95-8. DOI: 10.1016/j.jpag.2006.01.006 PMID: 1662696.
- Bakos O, Berglund L. Imperforate hymen and ruptured hematosalpinx: A case report with a review of the literature. J Adolesc Health. 1999 Mar;24(3):226-8. DOI:10.1016/s1054-139x(98)00077-9. PMID: 10195807.
- Diagnosis and Management of Hymenal Variants: ACOG Committee Opinion, Number 780. Obstet Gynecol. 2019 Jun;133(6):e372-e376. DOI: 10.1097/AOG.0000000000003283. PMID: 31135763.
- Rex S, Agarwal P. Pinhole hymen- A case report. IOSR Journal of Dental and Medical Sciences. 2019 November;18(11) Ser.7:01-04. DOI: 10.9790/0853-1811070104
- Segal TR, Fried WB, Krim EY, Parikh D, Rosenfeld DL. Treatment of microperforate hymen with serial dilation: a novel approach. J Pediatr Adolesc Gynecol. 2015 Apr; 28(2):e21-2. DOI:10.1016/j.jpag.2014.06.001. Epub 2014 Jun 7. PMID: 25444056.