Article / Short Communication
eclaireMD Foundation, USA
Gerald C. Hsu, eclaireMD Foundation, USA
17 June 2020 ; 5 July 2020
This paper describes qualitatively how the author has assisted a patient with psychological disorders, specifically borderline personality disorder (BPD), during this COVID-19 epidemic.
The author is a medical research scientist in the field of psychological disorders, metabolism, and endocrinology with a specialty in diabetes and its complications. He is also a professionally trained mathematician, physicist, and engineer. The patient in this case study is a 40-year-old female with BPD.
The author eluded the 2003 SARS threat in China and Taiwan. In early January 2020, when the strange “Wuhan pneumonia” rumors suddenly appeared on certain Asian news networks, he immediately recognized the danger associated with this newly found virus. He then started his “self-quarantine” in the United States on 1/19/2020, much earlier than the majority of Europeans and Americans who became aware of its potential damage and severity.
Over these past 106 days, the author has maintained his personal contacts with this patient using the Internet only.
From [1] COVID-19 is a disease caused by SARS-CoV-2 virus which uses ACE-2 for cell entry. Currently, we thought that it is spread through respiratory droplets, though the transmission is still under investigation. Also, the virus has been found in blood and stool. Figure 1 shows that COVID-19 is a spectrum of diseases. Approximately 80% of confirmed cases are uncomplicated SARS-CoV-2 infection which may lead to mild pneumonia. About 15% would lead into severe pneumonia, with the remaining 5% ending up as acute respiratory distress syndrome (ARDS). Incidentally, this 5% percentage just falls into the range for the current death rate of COVID-19, which is about 4% to 10%.

Figure 1: COVID-19 information (Reference 1)
The author’s first rule is that he does not trust any governments’ statements regarding this virus. Most politicians are concerned more about politics, economics, or even “saving face” and not relying on scientific truths and medical facts. Of course, there are still lots of scientific facts that need to be uncovered through scientific and medical professionals. As a scientist, the author believes that decisions related to human life should only be based on scientific and medical knowledge along with experiences. Therefore, he decided to conduct his own data analysis (a sample analysis shown in Figure 2). He does not need any complex equations or fancy mathematical models to analyze COVID-19, but he must look into the situation from “correct” cutting-angles or entry-points without any distorted facts. In this virus-fighting business, having correct information is our first important battlefield; otherwise, data analysis results would end up with what computer scientists consider as “garbage in leads to garbage out”.
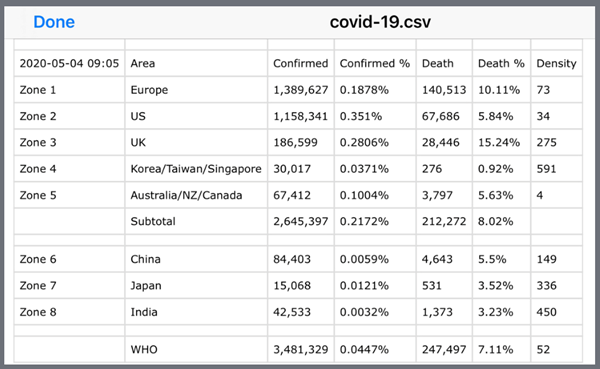
Figure 2:The author’s own partial data analysis of COVID-19
The spread of this disease depends mainly on the physical contact among people. Therefore, the population density is his first key factor. The combined inhabitants of China and India make up 38% of the world’s total population, and both of their data reliability and accuracy are questionable due to different reasons. This is why he chose not to look into the data provided by the World Health Organization (WHO). Furthermore, he did not look at the confirmed case “numbers”, but rather focused on the confirmed case “percentages” (i.e. confirmed case number divided by population). This confirmed case percentage could offer a better and clearer picture regarding whether that particular country was hiding the truth or providing inaccurate numbers. Of course, both of the confirmed case numbers and percentages are reflecting the availability and reliability of the virus testing kits. Specifically, he discovered that certain nations hide the truth by controlling the data “influx”, for example, by reducing the number of confirmed cases through different layers of government bureaucracy, reporting an inaccurate number, or refusing additional tests to be performed on the population. However, most underdeveloped or some developing nations, they are indeed in a situation of short supply of virus test kits.
Ironically, he discovered that the death percentages among different nations (death number divided by confirmed number) were quite consistent from each other, in a range between 4% to 10%. This death rate usually reflects that particular country’s healthcare conditions and medical resources in terms of their facility availability and expertise level. Another non-related historical event regarding the death rate is the “Iwo Jima” campaigns of the Pacific War had a 6.2% death rate over 36 days of battles (6,800 out of 110,000 soldiers).
Fearing possible death caused by COVID-19, being bored with quarantined life, maintaining social-distancing with outsiders, and having school-aged children at home for an extended period can cause a normal person to be “crazy”. These restrictions for patients with existing psychological disorder conditions such as BPD can exacerbate their symptoms. Most BPD victims had severe abandonment in their childhood. In addition, they may have been exposed to some emotional, verbal, and/or physical abuse. During this COVID-19 period, this group of patients needs extra emotional care and love to cope with their “flash back” memories which could create more anxieties and emotional mood swings. Not only would they feel more stressed, they also transfer stress to their loved ones and create a life pattern similar to “walking on eggshells”.
Figure 2 shows the author’s own data analysis of COVID-19. He focuses on zones (a single nation or an area with multiple nations) having transparent information, such as the US, UK, and Europe. Within Zones 1, 2, and 3, including Europe, US, and UK, he found a confirmation percentage of 0.18% to 0.35% and a death rate of 5.8% to 10.1%. With regard to this virus death percentage, most countries in the world have a similar death rate percentage of about 4% to 10%. Two exceptionally well-controlled zones are: nations with dense populations with 591 people per square km (Zone 4) such as Taiwan, South Korea, and Singapore have 0.037% confirmation rate with a 0.92% death rate; and nations with sparse populations with 4 people per square km (Zone 5) such as Canada, Australia, and New Zealand have 0.1% confirmation rate with a 5.63% death rate. As a caveat, he could easily determine from his analysis which nations were hiding the truth about their confirmed case numbers or distorting the facts. For example, 3 particular nations’ confirmed case percentages are extremely low, 0.003%, 0.006%, and 0.012%.
Once he developed his information of confirmation rate and death rate, he then tried to decipher the death rates associated with the senior age groups (Figure 3). Although different countries or cities have presented different death rate comparison results between the older age group (>70 years old) versus the younger age group (<40 years old), the general idea is consistent. For a senior person, who has existing chronic diseases and history of complications, would have an extremely high death rate in the range of several tenth fold.
This particular patient in this article has suffered from BPD since her childhood. The following paragraphs list her behaviors, stimulators, and treatments (Figures 3, 4 and 5):
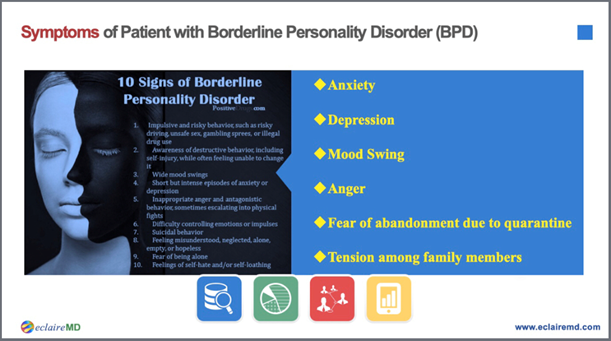
Figure 3: Symptoms of BPD during COVID-19 Epidemic
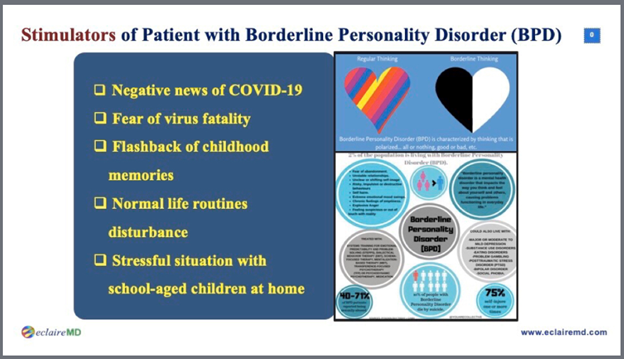
Figure 4: Stimulators of BPD during COVID-19 Epidemic
Figure 5: Treatments of BPD during COVID-19 Epidemic
- Abnormal behaviors: including anxiety, depression, mood swings, anger, and fear of abandonment.
- Possible stimulators: including negative news of the virus, fear of mortality of COVID-19, flashbacks, disturbed normal routine life pattern, school-aged children staying at home for an extended period.
- On-going treatments: including verbal expression of care and love, non-abandonment reassurance, additional financial assistance for increased cost of online livelihood items, and telemedicine with a remote psychotherapist.
As a result, this patient is living a “calmer” life during COVID-19 epidemic.
Borderline personality disorder is a life-time issue and it cannot be cured. Childhood abandonment and long-term emotional abuse has already caused “permanent” damage and emotional scars on the patient’s personality and behaviors. Showing love and care by her loved ones can definitely comfort her emotional mood swings. For this clinical case, it took many years to earn the patient’s partial trust and conditional acceptance. How could we blame a young child, who needed her parents’ love the most when they abandoned her both emotionally and physically? When a new traumatized event suddenly occurs later in her life, such as the life-threatening COVID-19 epidemic, it brought back a fearful feeling or some vivid bad memories or images. This situation is exceedingly difficult for a psychological disorder patient to cope with. Only unconditional love and emotional care supplemented with patience, persistence, and real actions can pacify and emotionally help this patient, whether during the COVID-19 period or not.
COVID-19 is more than 100 times worse than SARS in 2003, in terms of its spreading speed and scope, mortality rate, and emotional impact on the world population. People belonging to the “weaker” groups, such as the elderly, health problems (existing chronic diseases and history of complications), or psychological disorders, requiring additional attention, care and assistance. Unfortunately, some ridiculous opinions have appeared and circulated on the internet that COVID-19 can wipe out these weak people in order to reduce the government’s social welfare burden. Only an immoral person can think this way.
On the other hand, the author also saw positive signs of the human spirit when he read the following news:
- An elderly patient in New York volunteered his hospital bed to rescue a younger patient.
- 76,000 retired healthcare professionals went back to their old post to fight against the virus in New York City.
- 25,000 retired healthcare professionals signed up on the first day to go back to their old post to fight against the virus in California.
- Due to limited information, estimated thousands of healthcare professionals from all over China have already died in Wuhan to rescue COVID-19 patients.
This article is based on the author’s own medical knowledge and specific psychotherapy practices to protect certain patients, either physiological or psychological [2-4]. He hopes his academic knowledge from the past 20-years of medical research in the fields of psychology, endocrinology, and metabolism can help individuals with psychological disorders and chronic diseases to strengthen their metabolism and immunity to fight COVID-19 effectively. In addition, his self-learned knowledge of 9-years efforts in abnormal psychology and clinical experiences, from his five established psychotherapy centers, which helped 200 abused women, abandoned babies, and abused children. Hopefully, this can offer some guidance to provide emotional help or real assistance to other psychological disorders patients in order to survive through this difficult period.
- Dr. Joshua A Davis (2020) “COVID-19 at NYPH: What Are the Basics of the Disease, Symptoms and Risk Factors for Non-Critically Ill Patients?” New York-Presbyterian Hospital, New York video, April 17, 2020, https://www.vumedi.com/video/covid-19-at-nyph-what-are-thebasics-of-the-disease-symptoms-and-risk-factors-fornon-critically-ill/.
- Hsu Gerald C (2019) “Linkage among metabolism, immune system, and various diseases using GH-Method:math-physical medicine (MPM)” No. 235.
- Hsu Gerald C (2019) “Using GH-Method: mathphysical medicine, mentality-personality modeling, and segmentation pattern analysis to compare two clinic cases about linkage between T2D patient’s psychological behaviour and physiological characteristics” No. 72.
- Hsu Gerald C (2019) “Progressive behavior modification for diabetes patients based on GH-MPM Method (mathphysical medicine and mentality-personality modeling) and psychological & physiological linkage pattern analysis” No. 75.