
Article / Systemic Review
1Department of Physical Therapy, Howard University, Washington DC, USA.
2Department of Physical Therapy, Washington DC, USA.
3Department of Occupational Therapy. Poznan University of Medical Sciences. Poland.
Iwona Kasior,
Department of Physical Therapy Howard University, Washington,
DC. USA
15 August 2024 ; 6 September 2024
Background: Over the decades, the prevalence of arthritis in the United States has skyrocketed. Arthritis is the most common cause of disability in the United States. According to the National Arthritis Data Workgroup, more than 22% of American adults (which is equivalent to over 52.5 million people) suffer from arthritis or a rheumatic condition. Of those diagnosed with arthritis, 7.3% of people are aged 18-44, 30.3% are 45-64 years old, and 49.7% are over the age of 65. Women are also more prone to developing this disease than men; 26% of women have been diagnosed with arthritis whereas 19.1% of men have been diagnosed with arthritis. Researchers estimated that by 2030, the number of people who will be diagnosed with arthritis will increase to 67 million. There are three most common types of arthritis, two of which will be the focus of this systematic literature review, these include osteoarthritis and rheumatoid arthritis. Osteoarthritis is characterized by degeneration of cartilage as well as bony overgrowth while rheumatoid arthritis, while rheumatoid arthritis is an autoimmune and inflammatory disease affecting the joints of the body. Peloid and balneotherapy dates to the ancient past. Humans searching for healing remedies in the surrounding nature, discovered the healing effects of heat, cold and radiation solar and mineral waters. Instinct and observation of the world paved the way for natural but effective ways to treat pain. This literature review will be focused on the effects of peloid and balneotherapy on reducing the symptoms of arthritis and thus improving quality of life.
Purpose: The purpose of this targeted systematic literature review is to examine the relationship between the treatment of peloid and balneotherapy on patients with arthritis in reducing pain, arthritic symptoms and increasing their quality of life.
Methodology: A literature search was conducted using PubMed, Google Scholar, CINAHL, Science Direct databases. The search terms included balneotherapy, peloid therapy, arthritis, rheumatoid arthritis, osteoarthritis, quality of life, rehabilitation, physical activity, and pain management. Inclusion criteria: 18-65 years, published within the last 10 years, interventions related to peloid and balneotherapy, or both. An evidence level of 2b or higher was required for the inclusion criteria. Exclusion criteria includes not evaluating interventions of interest and therapeutic interventions for arthritis which are not peloid or balneotherapy related. A total of five articles (n = 5) were included in this systematic literature review. The original search criteria yielded 61 research articles related to the topic, which were then screened with the inclusion criteria with a remaining of five articles which were utilized in this review.
Results: A systematic literature review of five studies was performed. Five clinical studies measured the effectiveness of balneotherapy and/or peloid therapy and there was significant difference between the groups in WOMAC pain, stiffness, and function scores and in the VAS.
Discussion: This review indicates that balneotherapy and peloid therapy were effective in reducing pain, stiffness, improving function as assessed by the WOMAC and VAS scores.
Osteoarthritis is one of the most common conditions of the motor organ and the second cause of disability after cardiovascular conditions. Patients most frequently suffer from pain and stiffness of joints, which decrease the capacity of locomotion, self-care, and quality of life. Osteoarthritis is the most common form of arthritis, caused when the protective cartilage at the ends of bones wears down over time. (Gomes et al., 2013).
This disorder is most common in the joints in hands, knees, hips, and spine, and major risk factors include aging, obesity, and injury. The wear and tear of joint cartilage causes symptoms that can progress overtime including pain, stiffness, tenderness, loss of flexibility, grating sensation, bone spurs, and swelling of the joints.
Rheumatoid arthritis (RA) is a form of arthritis characterized by joint pain and damage throughout the body. This is a chronic inflammatory autoimmune disease that can affect several organs and joints in the body (Gomes et al., 2013). Some symptoms of RA with regards to its effects on joints include pain, swelling, stiffness, deformity, and loss of function. One distinguishing feature of RA is that joint damage typically occurs on both sides of the body, meaning the same joints will be affected on both the right and left sides of the body. Risk factors include sex, with RA being more common in women, age, genetic predisposition, smoking, environmental exposures, and obesity.
In Europe, peloid and balneotherapy is implemented in people with osteoarthritis. These therapies are funded by the social security system in many other European countries (Forestier et al., 2009). Peloid therapy is a form of balneotherapy which is defined as therapeutic bathing. Peloid is a mud or clay that is used for therapeutic purposes. Peloid Therapy consists of dissolved and mineralized purified therapeutic mud, which is then applied to the body as a form of thermal therapy. (Gomes et al., 2013). Peloid is filled with decomposed aquatic plants which are given through hot temperatures. The goal of peloid therapy is to relax muscles, reduce swelling around muscle tension and to strengthen any anti-inflammatory activity that is occurring within the body. Peloid therapy is used to treat diseases such as rheumatism, inflammation, neuralgia, and obesity. (Maraver et al., 2021). The heat that is generated from the application of the peloid improves the blood circulation rate and local metabolism in the body. One form of peloid therapy that has traces back to thousands of years is a mud bath.
Peloid therapy is used as a form of management in arthritic conditions. Mud bath therapy has been reported to prevent arthritic conditions as well as manage them. (Kasapoğlu et al., 2017). Balneotherapy and mud bath therapy has effects on pain, quality of life and functional capacity. (Evcik et al., 2007). Along with improvements in pain and quality of life, spa therapy has also improved range of motion in patients with arthritic conditions. Patients who undergo treatment related to balneotherapy and peloid therapy have been shown to improve their physical activity and decrease their pain. (Varzaityte et al., 2019). Several studies have discussed the effectiveness of peloid and balneotherapy in regard to various arthritic conditions such as osteoarthritis and rheumatoid arthritis in comparison to other intervention methods such as pharmaceutical and rehabilitation. Studies have shown that peloid and balneotherapy have systemic activity that causes alterations in the biochemical and molecular parameters. (Espejo Antúnez et al., 2013). These biochemical and molecular parameters include reduced amounts of plasma tumor necrosis factor which is responsible for reducing pain and minimizing the inflammatory process found that the thermal stress from this intervention is due to thermal stress which stimulates the metabolism of chondrocytes, which produce joint cartilage protective effects. (Ibid.). Since there are no cures for rheumatoid arthritis, the treatment consists of different types of management to control pain, inflammation, stiffness and mobility. Studies have shown a low level of evidence of reduction in the number of tender joints. (Verhagen et al., 2015). Benedetti et al. evaluated the influence of physiotherapy based on sulfur baths on biomarkers of oxidation, inflammation, and decomposition of articular cartilage. According to the authors, sulfur baths used in patients with osteoarthritis are a useful complement to pharmacotherapy. In addition, the combination of sulfur baths and peloid treatment is recommended for preservation of therapeutic effects 25. Also, according to (Bellometti et al., 2010) regular peloid treatment with mineral baths reduces the use of painkillers and physiotherapy. (Bender et al., 2004).
Arthritis is a chronic illness with no cure to date. Treatment of this disease is generally focused on management of symptoms such as joint pain, stiffness, and discomfort for an overall increase in quality of life. More specifically, treatment options include medicinal interventions, physical therapy, and balneotherapy. Studies of the effects of balneotherapy on the progression of RA and severity of symptoms have generally been inconclusive. One study consisting of five trials showed that most trials reported positive findings with absolute improvement ranging up to 44 %, but due to methodological flaws this evidence is insufficient. (Ibid). A recent study involving 57 participants with RA evaluated the effectiveness of balneotherapy in the form of mineral baths; researchers noted some benefit of balneotherapy in overall improvement on a five-point scale at eight weeks of 54% (Verhagen et al., 2015). While research on the effectiveness of treating symptoms of RA with balneotherapy show some benefits in patient experience and pain management, there is no sufficient evidence to conclude balneotherapy is more effective than no treatment, or other currently used treatments.
Osteoarthritis is mostly treated with medications, physical therapy, and sometimes surgery to help reduce joint pain and maintain joint movement. Several studies have examined the general effects of balneotherapy in osteoarthritis patients and the management of pain control and other symptoms. One recent study has investigated the effects of mud packs and a mud bath therapy on the pain and functionality in patients with hand osteoarthritis. The study showed that in the second and sixth week of the study, there were statistically significant improvements in the parameters of hand grip strength, pinch strength, visual analogue scale, and the health assessment questionnaire. (Kasapoğlu Aksoy et al., 2017). Another recent study conducted on the effectiveness of balneotherapy on patients with knee osteoarthritis also indicated a significant improvement in the quality of life of the participants. (Antonelli et al., 2018). Balneotherapy with regards to the treatment of patients with osteoarthritis has shown positive effects on the treatment of symptoms and quality of life.
Overall, studies have shown that patients who were treated with forms of balneotherapy have experienced advantages in their course of their disease, especially in the long term. (Bender et al., 2004). This study found that mud baths with reduced pressure and temperature induced pain in patients with rheumatoid arthritis and normal subjects. (Ibid). Studies have found that plasma levels of β endorphin are raised after spending 2 hours of bathing, along with reduced serum concentrations of prostaglandin and leukotriene. (Bellometti et al., 2010). Prostaglandins cause vasodilation and studies have shown that these receptors contribute to the pathogenesis of rheumatoid arthritis. (McCoy et al., 2022). It is also important to note that along with this form of treatment, there is a placebo effect that may take place. Those who participate in spa and mud therapy receive not only reduced amounts of pain and improved function and mobility, but higher quality of life along with decreased levels of anxiety and depression. (Bender et al., 2004).
Studies have also demonstrated that the combination of mud pack and hot pack therapy can be effective in reducing arthritic symptoms in patients; this study evaluated the effect of mud therapy on serum YKL-40 levels in patients with knee osteoarthritis and found that YKl-40 levels were significantly high. (Güngen et al., 2012). YKL-40 is a glycoprotein produced by inflammatory stem cells which has shown to be elevated in neurodegenerative diseases associated with inflammatory processes. (Llorens et al., 2017). Thus, the presence of this glycoprotein seems to slow down the progression of osteoarthritis.
While balneotherapy has been used to manage chronic musculoskeletal diseases for a long period of time, it can be combined with other treatments such as physical exercise, hydrotherapy, and mud therapy. A recent study examined the effects of the combination of balneotherapy and physical therapy and found significant effects for improving pain, physical function, and gait speed in comparison to one of the interventions alone. (Onat et al., 2019).
Previous research has demonstrated a significant relationship between the use of peloid and balneotherapy on the treatment of arthritic conditions. Many of these studies have researched the benefits of peloid and balneotherapy on patients with arthritic conditions in reducing pain, reducing inflammation, increasing quality of life, and increasing overall mobility and range of motion. Research has supported the use of peloid and balneotherapy on patients who suffer from osteoarthritis.
The purpose of this study is to examine the relationship between the treatment of peloid and balneotherapy on patients with arthritis in reducing their symptoms and increasing their quality of life.
This study utilized a systematic literature review to answer the research questions above. The databases used for this literature review include PubMed, Google Scholar, CINAHL and ScienceDirect. The search limit criteria included articles published within the last 10 years. The search terms used were a combination of the following: balneotherapy, peloid therapy, arthritis, osteoarthritis, quality of life, rehabilitation, functional performance, physical activity, and pain management.
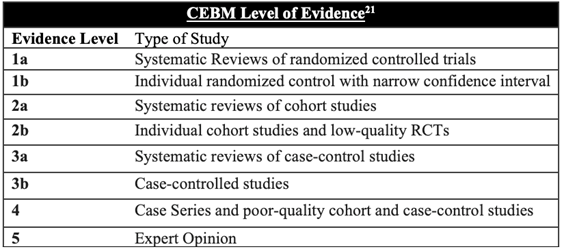
Search limit parameters were to only include articles published since 2011. The articles considered for this systematic review must be a level 2b or higher according to the CEBM criteria (Table 1). The articles must compare peloid or balneotherapy effects on people diagnosed with arthritis.
Using the search parameters abode, the initial search yielded 61 research articles (n=61). A review of the article titles and abstracts was performed, and articles were excluded if they did not evaluate the interventions of interest for arthritis which are not peloid or balneotherapy related. The remaining articles (n=5) met these criteria. Figure 1 summarizes the literature search and studies selection procedure for this systematic literature review.
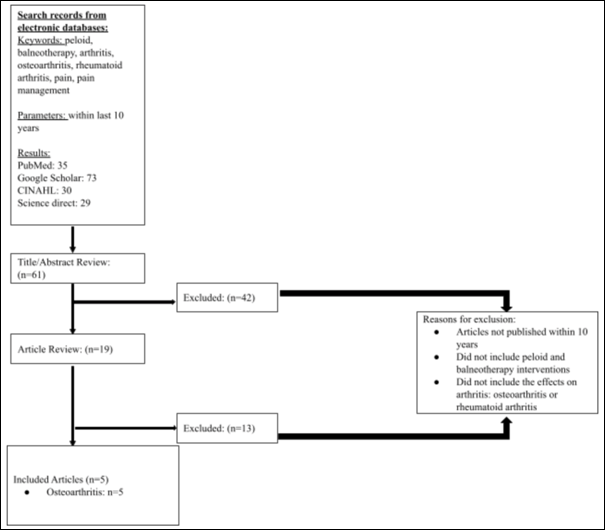
Figure 1: Literature Search and Exclusion Criteria
Three of the five research studies utilized the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) as shown in Figure 2. The WOMAC is a self-administered health status measure used in assessing pain, stiffness, and function in patients with osteoarthritis of the hip or knee. The areas of assessment for the WOMAC include activities of daily living, functional mobility, gait, general health, pain, and quality of life.
 Figure 2: The WOMAC Survey Form
Figure 2: The WOMAC Survey Form
Three of the five articles utilized the Visual Analogue Scale (VAS), which is a measurement instrument focused on characteristic or attitude that is believed to range across a continuum of values and can easily be directly measured (Gould et al., 2001), as shown in Figure 2. The scores are recorded by making a handwritten mark on a 10-cm line that represents a continuum between “no pain” and “worst pain.”
Literature screening and literature characteristics
The initial literature search identified 167, of which after title/abstract review and full text assessment, five studies were considered eligible for inclusion. The main characteristics of all the included studies are summarized in Table 2.
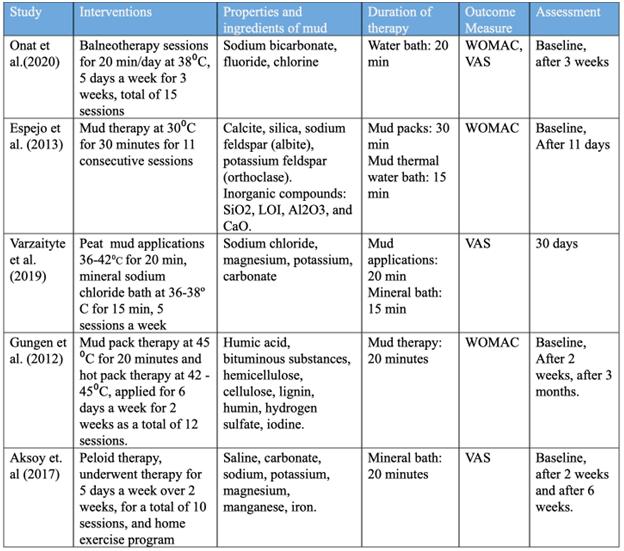
Table 2: The characteristics of studies included in the systematic review
There are three studies in which the treatment approach included mud therapy and in three studies the treatment approach was balneotherapy. In one of the studies, the treatment approach was mudpack therapy combined with balneotherapy).
Among the five studies, three of which utilized the WOMAC as an outcome measure while three studies utilized the VAS as an outcome measure. The result of the studies which used WOMAC as an outcome indicate that balneotherapy and mud therapy improve the symptoms of osteoarthritis. The result of the studies which used the VAS as an outcome also indicated that balneotherapy and mud therapy improved pain, stiffness, and physical function. One study utilized both the WOMAC and the VAS as an outcome.
The five articles that analyzed the effectiveness of balneotherapy and peloid therapy on arthritis were (Onat et al., 2015; Espejo et al., 2013; Varzaityte et al., 2019; Gungen et al., 2012; Aksoy et. al., 2017). As shown in Table 3, five out of the five articles analyzed the effectiveness of balneotherapy and peloid therapy on patients with osteoarthritis while the remaining article analyzed the effectiveness on patients with rheumatoid arthritis. All five articles demonstrated a statistically significant difference in the treatment use of balneotherapy and/or peloid therapy on reducing symptoms of osteoarthritis and increasing quality of life.
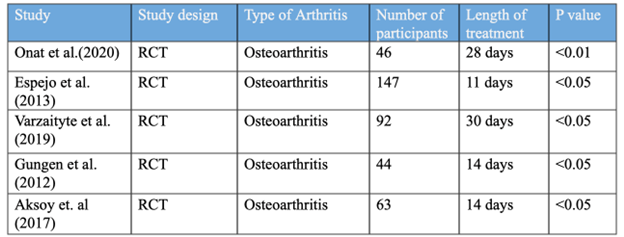 Table 3: Statistical analysis of research studies
Table 3: Statistical analysis of research studies
The clinical studies included in this systematic literature review consisted of five balneotherapy and peloid therapy cases in total. Among the included studies, the smallest sample size was n=44 and the largest sample size was n=147. The shortest duration of the given intervention was 11 days while the longest was 30 days.
This systematic literature review included five clinical trial studies, three of which showed the effect of balneotherapy and three showed the effect of peloid therapy on pain relief, functional improvements, and quality of life improvement. The result of this literature review favored balneotherapy and peloid therapeutic interventions compared to standard treatment for reducing symptoms of arthritis which includes pain relief, stiffness, quality of life and functional improvements. Findings demonstrated that the use of balneological and peloid interventions such as hot mineral baths or mud/peloid treatments improved pain and stiffness due to the chemical properties of these therapeutic modalities.
The effectiveness of balneotherapy and peloid therapy can be explained due to the thermal, mechanical, and chemical effects of the intervention. The thermal effects lead to an increase of blood flow and vasodilation which results in increased blood supply and the removal of nociceptive elements. (Halevy et al., 2001). Thus, the application of heat enhances the repair of the inflamed tissues, as seen in rheumatoid arthritis. The application of thermal stimuli also alters pain sensation, as shown in the gate control theory. The application of heat has been shown to induce sedation and muscle relaxation which allows for increased joint mobility. (Kuczera et al., 1996).
Immersing affected body parts in mineralized water bath allows for easier joint mobility along with the facilitation of muscle relaxation. (Lange et al., 2006). In return, the increase in joint mobility and muscle relaxation has been shown to alleviate arthritic pain symptoms and thus increase quality of life. While this systematic review yielded significant results, continued research is needed to establish a strong relationship between balneotherapy and peloid interventions in arthritic symptoms, functional mobility, and overall quality of life.
A strength of this systematic review is the inclusion of randomized controlled design (RCT) studies which allowed for the minimization of selection bias. However, the limitations of this study include the small sample sizes, the decreased available research that meets the criteria, variability in the outcome measures used such as the VAS and WOMAC. The limitations also include the limited research available which reduced the generalizability of this systematic review.
Further research studies are needed to establish the relationship between the short term and long-term effects of balneotherapy and peloid therapy on arthritic conditions. The authors recommend continued research that emphasizes improved methodological quality, outcome measures, increased sample size, increased follow up assessment of the interventions to understand the effectiveness of this intervention.
In conclusion, this systematic literature review suggests that there is a positive role in the use of balneotherapy and mud therapy in the treatment of osteoarthritis; these studies demonstrate that there is a significant reduction in pain and stiffness and improvement of quality of life. However, further research is needed to identify the strength of the relationship between the uses of balneotherapy and peloid therapy on arthritis along with the long-term effects of these interventions.
-
-
-
- Gomes, C., Carretero, M. I., Pozo, M., F., Maraver, P., Cantista, F., Armijo, J. L., & Legido, F. (2013). Peloids and pelotherapy: Historical evolution, classification and glossary, Applied Clay Science. 75(76), 28-38. DOI: http://dx.doi.org/10.1016/j.clay.2013.02.008
- Forestier, R., Desfour, H., Tessier, J.-M., Françon, A., Foote, A. M., Genty, C., Rolland C., Roques, C.-F., & Bosson J.-L., (2010). Spa therapy in the treatment of knee osteoarthritis: a large randomized multicenter trial, Annals of the Rheumatic Diseases, 69(4), 660–665. https://doi.org/10.1136/ard.2009.113209, 2-s2.0-77950303760.
- Maraver, F., Armijo, F., Fernandez-Toran, M. A., Armijo, O., Ejeda, M.J., Vazquez, I., Corvillo, I., &Torres-Piles, S. (2021). Peloids as Thermotherapeutic Agents. International Journal of Environmental Research and Public Health, 18(4),1965. DOI: https://doi.org/10.3390/ijerph18041965
- Kasapoğlu Aksoy, M., Altan, L., Eröksüz, R., & Metin Ökmen, B. (2017). The efficacy of peloid therapy in management of hand osteoarthritis: A pilot study. International Journal of Biometeorology, 61(12), 2145-2152. DOI: https://doi.org/10.1007/s00484-017-1419-9
- Evcik, D., Kavuncu, V., Yeter, A., & Yigit, I. (2007). The efficacy of balneotherapy and mud-pack therapy in patients with knee osteoarthritis. Joint Bone Spine, 74(1), 60-65. DOI: https://doi.org/10.1016/j.jbspin.2006.03.009
- Varzaityte, L., Kubilius, R., Rapoliene, L., Bartuseviciute, R., Balcius, A., Ramanauskas, K., & Nedzelskiene, I. (2019). The effect of balneotherapy and peloid therapy on changes in the functional state of patients with knee joint osteoarthritis: a randomized, controlled, single-blind pilot study. International Journal of Biometeorology, 64(6),955-964. https://doi.org/10.1007/s00484-019-01785-z
- Espejo Antúnez, L., Caro Puértolas, B., Ibáñez Burgos, B., Porto Payán, J.M, & Torres Piles, S.T. (2013). Effects of Mud Therapy on Perceived Pain and Quality of Life Related to Health in Patients with Knee Osteoarthritis. Reumatología Clínica (English Edition), 9(3), 156-160. DOI: https://doi.org/10.1007/s00484-019-01785-z
- Ibid.
- Verhagen, A. P, Bierma-Zeinstra, S. M., Boers, M., & Cardoso, R. J. (2015). Balneotherapy (or spa therapy) for rheumatoid arthritis. Cochrane Database Syst Rev, 4(4), CD000518. DOI:http://dx.doi.org/10.1002/14651858.CD000518.pub2
- Bellometti, S., Bertocco, E., & Galzigna, L. (2010). MPT does not modify lipid serum levels. Focus on Alternative and Complementary Therapies,3(4), 182-182. DOI: https://doi.org/10.1111/j.2042-7166.1998.tb00911.x
- Bender, T., Karagülle, Z., Bálint, G. P., Gutenbrunner, C., Bálint, P.V., & Sukenik, S. (2004). Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatology International, 25(3), 220-224. DOI: https://doi.org/10.1007/s00296-004-0487-4
- Ibid.
- Kasapoğlu Aksoy, M., Altan, L., Eröksüz, R., & Metin Ökmen, B. (2017). The efficacy of peloid therapy in management of hand osteoarthritis: A pilot study. International Journal of Biometeorology, 61(12), 2145-2152. DOI: https://doi.org/10.1007/s00484-017-1419-9
- Antonelli, M., Donelli, D., & Fioravanti, A. (2018). Effects of balneotherapy and spa therapy on quality of life of patients with knee osteoarthritis: a systematic review and meta-analysis. Rheumatol Int, 38(10), 1807-1824. DOI: doi:10.1007/s00296-018-4081-6
- Bender, T., Karagülle, Z., Bálint, G. P., Gutenbrunner, C., Bálint, P.V., & Sukenik, S. (2004). Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatology International, 25(3), 220-224. DOI: https://doi.org/10.1007/s00296-004-0487-4
- Ibid.
- McCoy, J. M., Wicks, J. R., & Audoly, L. P. (2002). The role of prostaglandin E2 receptors in the pathogenesis of rheumatoid arthritis. J Clin Invest, 110(5), 651-658. DOI: https://doi.org/10.1172/jci15528
- Güngen, G., Ardic, F., Fındıkoğlu, G., & Rota, S. (2012). The effect of mud pack therapy on serum YKL-40 and hsCRP levels in patients with knee osteoarthritis. Rheumatol Int, 32(5), 1235-1244. DOI: 10.1007/s00296-010-1727-4
- Llorens, F., Thüne, K., Tahir, W. Kanata, E., Diaz-Lucena, D., Xanthopoulos, K., Kanata, E., Pleschka, C., Garcia-Esparcia, P., Schmitz, M., Ozbay, D., Correia, S., Correia, A., Milosevic, L., Andréoletti. O., Fernández-Borges, N., Vorberg, M. L., Glatzel. M., & Sklaviadis, T. (2017). YKL-40 in the brain and cerebrospinal fluid of neurodegenerative dementias. Mol Neurodegeneration, 12, 83. https://molecularneurodegeneration.biomedcentral.com/articles/10.1186/s13024-017-0226-4
- Onat, S. S., Tasoglu, o., Zuhal, O., & Guneri, d. f. (2015). ŞŞAHİN. Balneotherapy in the treatment of knee osteoarthritis: A controlled study. Archives of Rheumatology, 30(4), 292-297. DOI:http://dx.doi.org/10.5606/ArchRheumatol.2015.5484
- Halevy, S., Giryes, H., Friger, M., Grossman, N., Karpas, Z., Sarov, B., & Sukenik, S. (2001). The role of trace elements in psoriatic patients undergoing balneotherapy with Dead Sea bath salt. Isr Med Assoc J, 3(11), 828-832. https://pubmed.ncbi.nlm.nih.gov/11729578/
- Kuczera, M., & Kokot, F. (1996). Wp-yw leczenia uzdrowiskowego na uk-ad endokrynny. I: Hormony reakcji stresowej [Effect of spa therapy on the endocrine system. I. Stress reaction hormones]. Pol Arch Med Wewn, 95(1),11-20. https://pubmed.ncbi.nlm.nih.gov/8677189/
- Lange, U., Müller-Ladner, U., & Schmidt, K. L. (2006). Balneotherapy in rheumatic diseases–an overview of novel and known aspects. Rheumatol Int, 26(6), 497-499. https://doi.org/10.1007/s00296-005-0019-x
- Benedetti, S., Canino, C., Tonti, G., Medda, V., Calcaterra, P., Nappi, G., Salaffi, F., & Canestrari, F. (2010). Biomarkers of oxidation, inflammation and cartilage degradation in osteoarthritis patients undergoing sulfur-based spa therapies, Clinical Biochemistry, 43(12), 973–978. 2-s2.0-77954315229, https://doi.org/10.1016/j.clinbiochem.2010.05.004.
-
-