
Article / Case Report
Department of Surgery, Tokushima Red Cross Hospital 103 Irinokuchi komatsushima-Cho, Komatsushima city, Tokushima, JAPAN, 773-8502.
Hisashi Ishikura,
Department of Surgery,
Tokushima Red Cross Hospital 103 Irinokuchi Komatsushimacho, Komatsushima City,
Tokushima, JAPAN
14 January 2025 ; 29 January 2025
Citation: Ishikura, H. et al. (2025). Use of Autologous Platelet-Rich Plasma for Treating Spontaneous Pneumothorax in Young Adults. J Medical Case Repo 7(1):1-4. DOI : https://doi.org/10.47485/2767-5416.1099
We used autologous platelet-rich plasma (PRP) as an adhesive in the lungs of a young patient with spontaneous pneumothorax. Because PRP is prepared from the patient’s own blood, the patient is not at risk for new infections or rejection. Under general anesthesia, approximately 100 mL of peripheral blood was collected and centrifuged repeatedly to create PRP, and autologous thrombin was created in a separate container. Regenerative oxidized cellulose membrane (ROCM) is applied to the entire upper lobe, including the staple line. The sheet is fixed with PRP and autologous thrombin is sprayed onto the sheet. As an alternative to fibrin glue, it may be of particular benefit to younger patients.
In young patients, pleural coverage with a polyglycolic acid sheet (PGA) and fibrin glue would be more effective than no coverage in preventing postoperative recurrence of spontaneous pneumothorax. The meta-analysis based on a European guideline published in 2015 showed that PGA coverage could help prevent pneumothorax recurrence (Kadomatsu et al., 2021). In clinical practice, especially in Asian countries, the visceral pleura around the staple line is reinforced. Kurihara et al. reported that applying ROCM with fibrin glue to the staple line reduced the postoperative recurrence rate and that visceral pleural coverage with ROCM and fibrin glue induced pleural thickening in animal experiments (Kurihara et al., 2016). In basic experiments, Sakai et al. reported that fibrin glue, as well as the application of PGA and ROCM, is necessary for visceral pleural repair (Sakai et al., 2018). However, the safety of fibrin glue, which is a bovine- or human-derived blood product, is unclear with regard to unknown viral infections and immunologic reactions. Blood products, such as fibrin glue may increase the risk transmission of human parvovirus B19, unknown viral infections, and allergic reactions (Kawamura et al., 2002). In particular, the incidence of spontaneous pneumothorax peaks in the teens and twenties, and people of those ages tend to refuse treatment with blood transfusions.
Autologous platelet-rich plasma (PRP) has various tissue repair–promoting properties, including many growth factors, and is used mainly in the fields of cosmetic surgery and dentistry. We used PRP as an adhesive in the lungs of a young patient with spontaneous pneumothorax who requested its use after sufficient explanation.
While the patient was under general anesthesia, approximately 100 mL of peripheral blood was collected and stored in an autologous blood component collection bag. From a side tube, 10 mL of blood was collected separately for autologous thrombin preparation. The autologous blood was centrifuged at low speed (1000 rpm) for 10 min; then the plasma was transferred to a small bag. The plasma was centrifuged at 3000 rpm for 5 min to adjust the content volume to approximately 4 mL; then the platelets were resuspended. The bag of platelets was shaken for 5–10 min to obtain PRP, and the platelets were counted. Using a syringe, we collected calcium chloride and serum in a ratio of 1:3 to make autologous thrombin (Figure 1B, C). The PRP was collected from the PRP bag (Figure 1A), and the PRP and the serum and calcium chloride were aspirated into separate containers (Figure 1D).
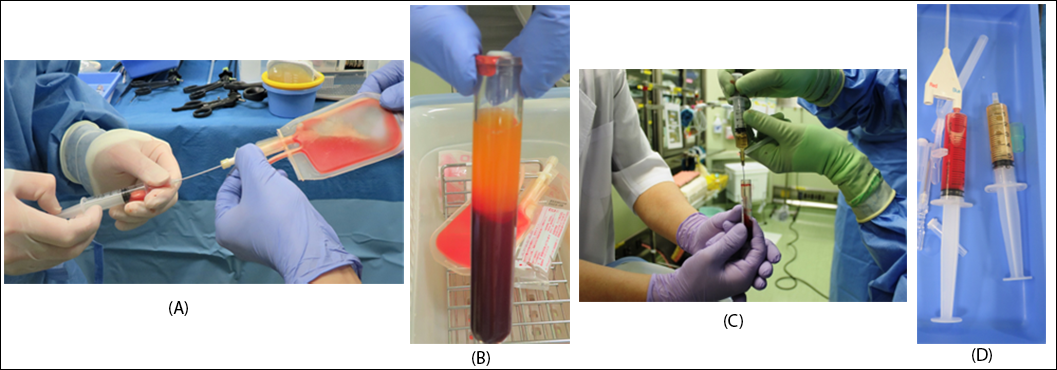 Figure 1: The operator collects into the syringe by clean operation Aspirate PRP (A) and serum(B,C) + calcium chloride separately (D) The PRP was collected from the PRP bag, and the PRP and the serum and calcium chloride were aspirated into separate containers.
Figure 1: The operator collects into the syringe by clean operation Aspirate PRP (A) and serum(B,C) + calcium chloride separately (D) The PRP was collected from the PRP bag, and the PRP and the serum and calcium chloride were aspirated into separate containers.
Since 2015, 32 patients who have undergone surgery for spontaneous pneumothorax have consented to receive PRP. The blebs are resected thoracoscopically with a stapling device. The entire upper lobe, including the staple line, is affixed with Regenerative oxidized cellulose membrane (ROCM), a plant-absorbable hemostatic agent made by oxidization of cellulose fibers obtained from wood pulp (Figure 2A) that we have used as a material to cover the pleura because it is inexpensive and does not cause adhesion easily (Uramoto & Tanaka, 2014). Then the sheet was fixed with PRP, and autologous thrombin was sprayed onto the sheet (Figure 2B).
All experiments were performed in accordance with relevant guidelines and regulations. Informed consent was obtained from all patients. This procedure has been approved by the hospital’s ethics committee (#253).
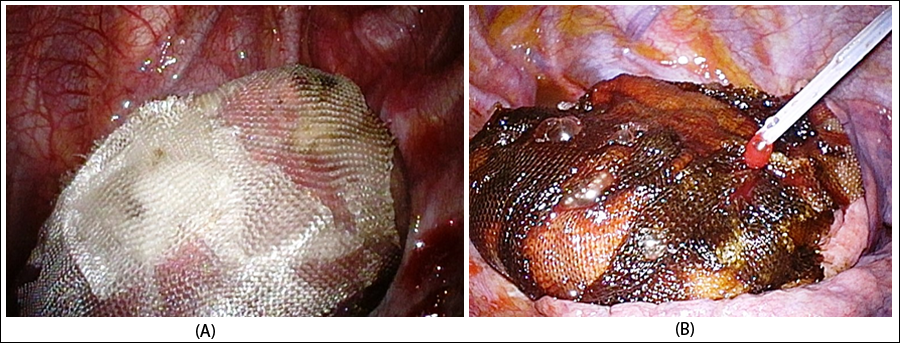 Figure 2: (A) Entire lung (upper lobe) covered with ROCM. (B) Apply PRP and then thrombin.
Figure 2: (A) Entire lung (upper lobe) covered with ROCM. (B) Apply PRP and then thrombin.
Among our 32 patients, the mean platelet count was 22.5 × 10⁴/μL; with PRP, it was 170.5 × 10⁴/μL, more than 7.5 times higher. Patients’ mean age was 21 years (range: 15–31 years), and the mean operative time was 79.0 min (range: 60–154 min). Two patients experienced recurrences of spontaneous pneumothorax, none of which could be attributed to PRP. Of the two cases, one was a recurrent surgery 9 months later due to a newborn bra, and the other was a recurrence one week later, which we believe was caused by an oversight due to an unknown leak site in the first surgery.
In PRP, the concentration of platelets is three to five times higher than normal. Recent basic research on the mechanism of wound healing has revealed that growth factors released from platelets play an important role in the initial wound healing process (Garg, 1999). In 1998, Marx et al. reported that mixing PRP into bone grafts promoted bone formation; this led to study of its direct application to tissue (Marx et al., 1998). After that, PRP attracted attention in the fields of regenerative medicine and wound healing, and it is now used not only for bones but also for soft tissues.
Growth factors in platelets are not released until the platelets are activated (coagulation reaction begins). The most common method of activating platelets is the addition of thrombin and calcium chloride. As mentioned, PRP not only can activate tissues through the physiological activities of various cytokines contained in platelets but also can have hemostatic, tissue adhesion, and wound-covering effects through its action as a fibrin/platelet glue.
In a report of PRP application to the lungs, pleural proliferation around PRP was confirmed (Kimura et al., 2008) (Kimura et al., 2017). They have used PRP from autologous blood, considering the cost to be more efficient, safe and economical than commercial fibrin glue. Their conclusion is that PGA sheet and PRP may effectively covering new bullous formation closing the staple lines.
Among the histopathological features, mesothelial cells and giant cells are thought to support the robust visceral pleura. Furthermore, by supplying sufficient nutrients from blood components to cells repaired by various growth factors, it is thought to be effective in preventing recurrence of pneumothorax and treating refractory pulmonary leakage. Ozawa et al. suggested that it is necessary to reinforce fixation of visceral pleura and ORC mesh with fibrin glue or autologous blood, because ORC mesh is broken down in the thoracic cavity (Ozawa et al., 2018).
Autogenous PRP has less risk of infections and allergic reactions and has abundant growth factors for tissue regeneration, which make it particularly effective for the prevention of recurrence of spontaneous pneumothorax. We suggest that PRP and ROCM are useful for postoperative prevention of recurrence of spontaneous pneumothorax.
Because autologous PRP is prepared from the patient’s own blood, the patient is not at risk for new infections or rejection, and PRP can be used safely and inexpensively. As an alternative to fibrin glue, which is currently in wide use, it may be of particular benefit to younger patients.
We would like to thank Mr. K. Matsushita and Ms. Y. Bando in the Examination Department for their cooperation in the protocol and the actual procedure.
- Kadomatsu, Y., Fukui, T., Mori, S., Chen-Yoshikawa, T. F., & Wakai, K. (2021). Polyglycolic acid sheet covering to prevent recurrence after surgery for spontaneous pneumothorax: a meta-analysis. Sci Rep, 11, 3392. DOI: https://doi.org/10.1038/s41598-021-83103-5
- Kurihara, M., Mizobuchi, T., Kataoka, H., Sato, T., Kumasaka, T., Ebana, H., Yamanaka, S., Endo, R., Miyahashira, S., Shinya, N., & Seyama K. (2016). A total pleural covering for lymphangioleiomyomatosis prevents pneumothorax recurrence. PLoS One, 11(9), e0163637. DOI: https://doi.org/10.1371/journal.pone.0163637
- Sakai, T., Matsutani, N., Kanai, E., Yamauchi, Y., Uehara, H., Iinuma, H., & Kawamura, M. (2018). Efficacy of a sheet combined with fibrin glue in repair of pleural defect at the early phase after lung surgery in a canine model. Gen Thorac Cardiovasc Surg, 66(2), 103–107. DOI: https://doi.org/10.1007/s11748-017-0857-y
- Kawamura, M., Sawafuji, M., Watanabe, M., Horinouchi, H., & Kobayashi, K. (2002). Frequency of transmission of human parvovirus B19 infection by fibrin sealant used during thoracic surgery. Ann Thorac Surg, 73(4), 1098-100. DOI: https://doi.org/10.1016/s0003-4975(02)03415-x
- Uramoto, H., & Tanaka, F. (2014). What is an appropriate material to use with a covering technique to prevent the recurrence of spontaneous pneumothorax?. Journal of Cardiothoracic Surgery, 9, 74. DOI: https://doi.org/10.1186/1749-8090-9-74
- Garg, A. K. (1999). Grafting Materials in Repair and Restoration. In S. E. Lynch, R. J. Genco, & R. E. Marx, (Eds.), Tissue Engineering: Applications in Maxillofacial Surgery and Periodontics (pp. 83-102). Quintessence Publishing, Illinois. https://www.scirp.org/reference/referencespapers?referenceid=2323685
- Marx, R. E., Carlson, E. R., Eichstaedt, R. M., Schimmele, S. R., Strauss, J. E., & Georgeff, K. R. (1998). Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 85(6), 638-46. DOI: https://doi.org/10.1016/s1079-2104(98)90029-4
- Kimura M, Kajiwara N, Taira M, et al. (2008). Basic study on pulmonary fistula closure approaches using platelet rich plasma (PRP). J Tokyo Med Univ, 66, 380-388.
- Kimura, M., Miyajima, K., Kono, T., Hayashi, A., Iwaya, K., & Ikeda, N. (2017). Effectiveness of Polyglycolic Acid Sheet Covering and Platelet-Rich Plasma after Video-Assisted Thoracic Surgery for Spontaneous Pneumothorax. Thorac Cardiovasc Surg, 65(1), 61-64. DOI: https://doi.org/10.1055/s-0035-1564448
Ozawa, Y., Sakai,M., & Ichimura, H. (2018). Covering the staple line with polyglycolic acid sheet versus oxidized regenerated cellulose mesh after thoracoscopic bullectomy for primary spontaneous pneumothorax. Gen Thorac Cardiovasc Surg, 66(7), 419-424. DOI: https://doi.org/10.1007/s11748-018-0927-9