









Article / Case Report
1NICU Consultant
2Head of department NICU Consultant Maternity children Hospital Makkah (MCH)
3NICU Consultant (MCH)
4NICU Consultant king Feisal specialist hospital Jeddah (KFSH)
5Gastroenterology consultant (MCH)
6Senior consultant Pediatric (MCH)
7NICU SPECIALIST (MCH)MAKKAH
8Pediatric Saudi board resident, Makkah (MCH)
Najia al hojaili
NICU Consultant
Maternity Children Hospital Makah
Saudi Arabia
30 November 2020 ; 14 December 2020
Meconium cyst in pre-term baby is rare. Meconium pseudo cyst is a complication of meconium peritonitis which is a sterile chemical peritonitis due to intrauterine bowel perforation. When the perforation in the intestine does not heal and communication with the cyst persist postnatal that can lead to cyst expansion, infection of the cyst or rupture of pseudo cyst. This is a case report of a neonate with rupture of meconium pseudo cyst causing perforation peritonitis [1].
Our case is preterm 32 weeks part of twins, cesarean section presented with huge abdominal distention diagnosed prenatal as meconium cyst.
Meconium cyst perforation is serious complication especially when was happened in preterm baby, and time of perforation.
It leads to chemical peritonitis which is fetal disease.
Meconium cyst can be diagnosed antenatal by us abdomen and managed very well postnatal any delay in diagnosis and management lead to serious complication like peritonitis.
The incidence is 1 in 30,000 live births
The proposed etiology for perforation:
- ischemia of the intestine
- mechanical obstruction like atresia,
- Volvulus, extrinsic congenital bands,
- Meconium ileus, internal hernias,
- intussusceptions, Meckel’s diverticulum,
- Hirschsprungs disease
32 Weeks product of LSCS twin with Apgar score6, 8, 9, 1st twin was distressed put on CPAP and load by caffeine.
2nd twins had severe abdominal distension, severe distress, immediately intubate in delivery room and shifted to NICU, put on MV but she was not maintaining saturation, shift to HVOV and called immediately pediatric surgery after x-ray
CBC showed leukocytosis
Blood gas shows severe respiratory acidosis
X-ray chest and abdomen: small lung volume and huge mass with small calcification
huge and massive cyst. Fluid turbid in in the intestinal cavity
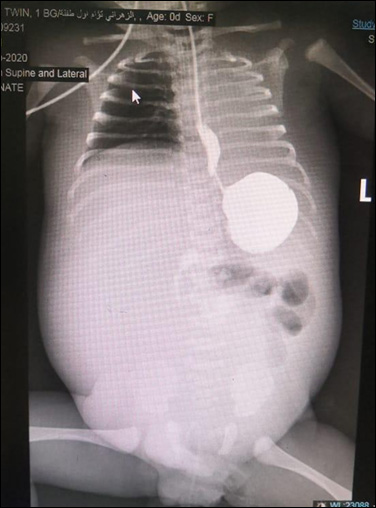
Figure 1: Gastrographene dye was done after removed of meconium cyst
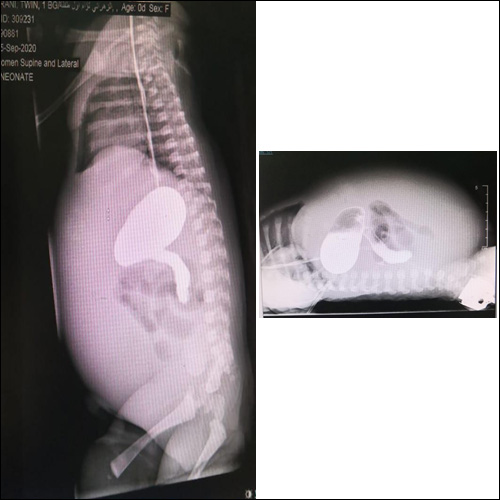
Figure 2: gastrographine dye reached to duodenum
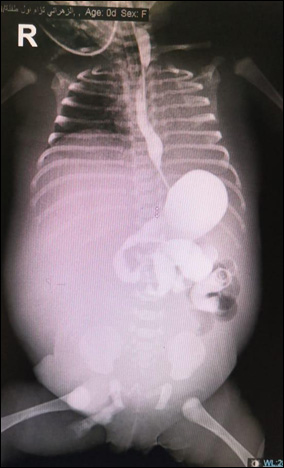
Gastrographene dye showed small intestine
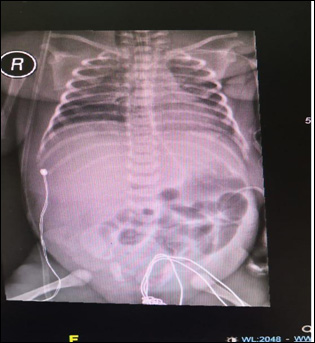
Post-operative PA Chest x-ray showed normal intestinal after removed meconium cyst
- RDS
- Respiratory Failure
- Rupture Meconium cyst with chemical peritonitis
- Intestinal tumor
Baby admitted immediately to NICU as case of respiratory distress and abdominal distension, pediatric surgery involved and asked for gastrographene dye was given and aspiration of the cyst under US guideline, aspiration showed meconium and pediatric surgery asked to prepared immediately for operation.
They found huge rupture meconium cyst and inflamed of peritoneal cavity
Post-operative vital signs were stable Temperature 37c, HR=140ppm, RR=assist ventilator Bp =Maintain
Baby covered by ampicillin and gentamycin and metronidazole and fentanyl and paracetamol for pain TPN 100ml/kg/day and blood gas and RBS monitoring.
Baby kept NPO for 10 days until stoma was working then started OGT breast milk protocol
Baby tolerated feeding but he had output drain from high stoma, he developed dehydration, so we increased fluid to 250ml/kg/day, and we gave him small amount of breast milk through OGT and the TPN
Baby was doing well extubated to Nasal cannula and increased milk gradually and he tolerated
Meconium is rare too appeared in preterm baby and when it appeared it associated by intrapartum problem.
Our case is preterm 32 weeks 2nd twin, weight 1.8 kg .1st twin 2.2 kg discharge with mother
No maternal illness, mother is young 25 years para 2 , 1st baby completely healthy .no consequently, no chronic illness in the family
Cystic fibrosis test was rolled out
Meconium cyst perforation is serious problem leads to chemical peritonitis and serious problem
Meconium cyst diagnosed antenatal by ultrasound and informed NICU for further management
Meconium cyst perforation if not taken immediately to surgery baby will suffered a lot like malabsorption, and screening for cystic fibrosis must be done in each case
No conflict
- Saleh N, Geipel A, Gembruch U, et al. (2009) Prenatal diagnosis and postnatal management of meconium peritonitis. J Perinat Med 37(5): 535–538.